
 显示该栏目以下所有产品
显示该栏目以下所有产品
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203



IOPI吞咽障碍评估和训练舌压仪-爱荷华口腔行为仪
IOPI吞咽障碍评估和训练舌压仪-爱荷华口腔行为仪(iowa oral performance instrument,IOPI), 可以客观地衡量评估和训练:舌头的力量和耐力;嘴唇的力量和耐力。
通过相应的措施和方式帮助参与治疗和研究影响吞咽、言语和吞咽障碍的医学专业人员和患者:客观地记录治疗的缺陷;诊断区分肌肉无力和运动控制问题;在等距口腔运动训练程序中提供生物反馈;通过展示肌肉运动疗法中取得的进展以此激励患者。
关于吞咽障碍评估和训练,舌压测量是一种简单的判断患者舌肌力的方法,研究证实,吞咽困难的患者都有不同程度的舌压降低现象,因此舌压可以作为一项评估吞咽功能、尤其是预测吞咽功能障碍的指标。其中,使用IOPI舌压仪-爱荷华口腔行为仪(iowa oral performance instrument,IOPI), 应用于测量舌的峰值压力及耐力,简便易用,且可获得较客观准确的数据,特别对脑卒中后吞咽障碍患者吞咽功能的评估,具有良好的评估意义,能够量化地反映卒中后吞咽障碍的程度和变化,同时,通过IOPI吞咽障碍评估和训练舌压仪的训练模式,可以很好地解决了脑卒中后吞咽功能障碍患者的舌肌、唇肌、颊肌的肌力和耐力训练;患者训练的情况还能及时通过IOPI训练处方记录表进行记录,以便对患者治疗前、后进行对比以观察疗效;IOPI主机上的灯光设置可对患者起到生物反馈的作用,生物反馈辅助功能也有利于患者的行为控制,研究显示,生物反馈能提高患者主动参与训练积极性,并能巩固疗效。
工作原理描述
- 测量力量强度
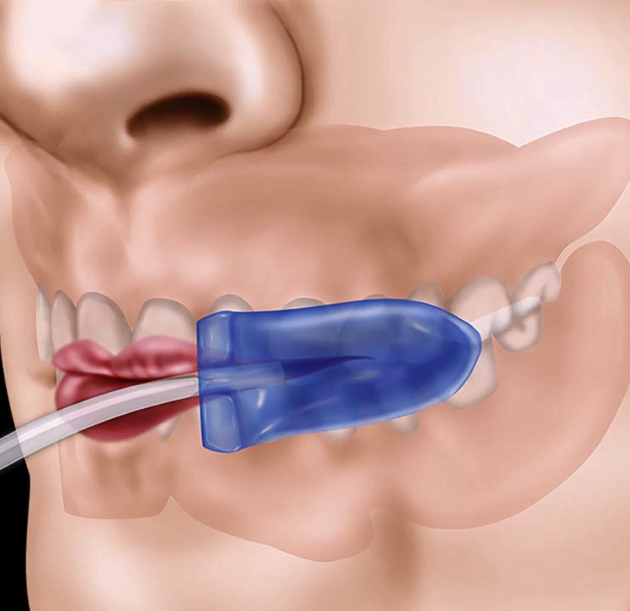
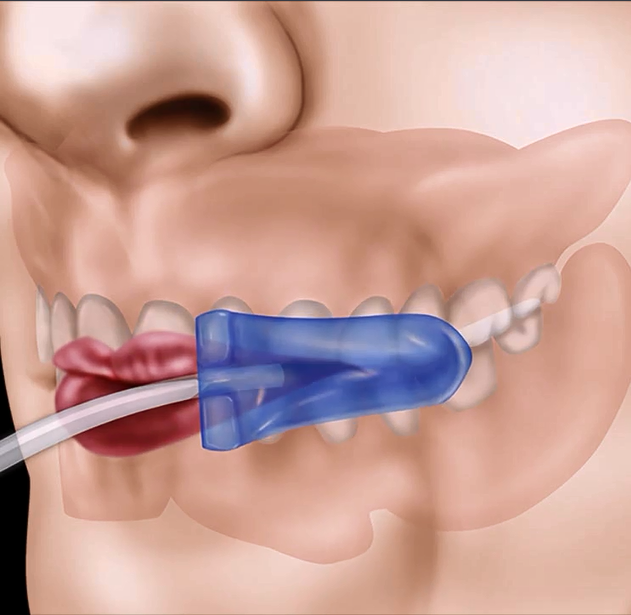
嘴唇的压力强度取决于嘴周围的圆周肌复合体的强度。正是这些肌肉的张力使嘴唇彼此紧压。标准压力球囊放在嘴角的嘴唇下方,受试患者将嘴唇合起,并尽可能用力撅起嘴唇产生的最大压力。
IOPI舌压仪的测量单位是基于国际公认的压力单位:千帕(kPa)。
- 测量耐力
IOPI舌压仪测量耐力值,通过量化患者能够保持其测试舌压力峰值50%的时长来实现。将目标模式中的目标值设置为患者测试压力峰值的50%,并计时患者可以保持顶部(绿色)灯亮起的时长。
- 运动疗法
设置目标值可以用代数表示:T = Pmax x(E / 100),其中:T =目标值,Pmax =最大舌压,E =作用力(%)
- 验证
舌力强度测量
- 临床重要性:了解患者的舌力强度在临床上有多种意义用途
如果舌头较弱,则可以开始强化舌头治疗;
如果舌头的力量是正常的,可以消除导致吞咽或语言问题,从而集中精力进行其他更有用的治疗;
证明患者的舌无力,因此加强锻炼是有需要的。这对于关心提供此类治疗的成本或收益来说可能很重要;
随着时间的推移评估增强舌力强度疗法的效果;
如果舌头的力量没有随着时间的推移而增加,那么也许患者没有进行规定的锻炼,或者训练做得还不够;
如果舌头的力量确实增加了,哪怕是增加了一点点,患者能看到具体的证据改善也会增加治疗信心;
锻炼患者的舌头。使用IOPI®进行舌运动可以为患者提供非常具体的“目标”,使其能够通过努力实现,并反馈改善情况。
- 利用生物反馈进行舌力训练
- 压力作为力量的衡量标准
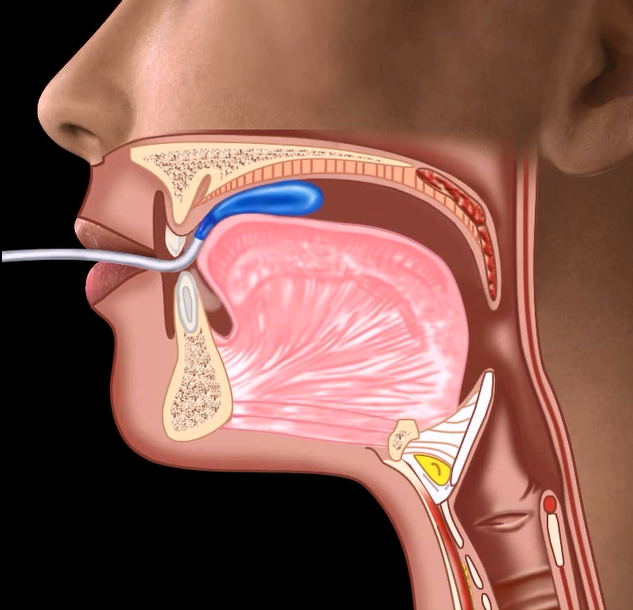
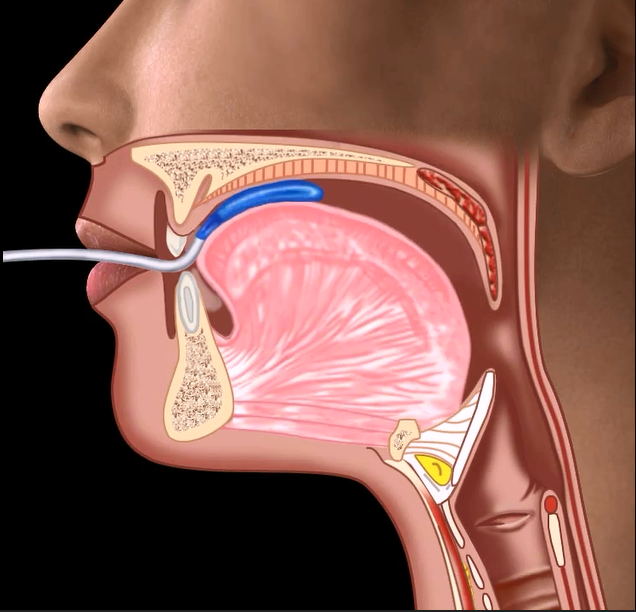
- 舌提升强度
大多数已发表的关于舌力强度的报告使用了IOPI舌压仪,压力泡囊位于“前”位。从许多不同的实验室和诊所获得了关于舌提升强度的信息表明了以下结论:
在同一个人身上重复测量舌头的力量是可靠的;
在报告没有吞咽障碍或语言问题的成年人群体中,舌力强度存在相当大的差异。但是,有一个明显的中心趋势,平均最大压力约为60千帕,范围为40-80千帕;
口腔吞咽困难患者的舌力强度明显低于正常人群;

唇部力量强度测量
- 为什么要测量嘴唇的力量?
- 唇部力量强度测量

IOPI吞咽障碍评估和训练舌压仪产品套装和配件(可按需选购)
- IOPI吞咽障碍评估和训练舌压仪(豪华套装),型号:PN 1-3100-DL
IOPI吞咽障碍评估和训练舌压仪(豪华套装),另外包含:IOPI报告生成单元1个;附件链接线1根
- IOPI吞咽障碍评估和训练舌压仪(标准套装),型号:PN 1-3100-SD
- IOPI吞咽障碍评估和训练舌压仪(训练套装),型号:PN 1-3200
- 标准舌压测量球囊(适用于,豪华套装和标准套装)—1盒10个,型号:PN 5-6010
- 训练用舌压测量球囊(适用于,训练套装)—1盒5个,型号:PN 5-6105
- 连接管(适用于,豪华套装和标准套装),型号:PN 5-0001
- IOPI报告生成单元,型号:PN 5-8101
- 橡胶面部模型,型号:PN 5-3001
- 患者进展数据表,15张,型号:PN 800-3102
- 舌头压力测量球囊定位表,型号:PN 800-3103
- 培训治疗师-患者使用说明;15张,型号:PN 800-3203
请根据需要选择购买相应IOPI吞咽障碍评估和训练舌压仪套装和所属配件。豪华套装特别附加配有的IOPI报告生成单元,可以从IOPI设备中提取数据,以详细查看所有执行的练习,并生成可打印的报表。
原装进口,产地美国
- 另外一款日本制造的性价比的舌压仪:JMS舌压测量计
- Barthel指数(BI)评定量表详解 —— 日常生活活动能力评估工具的标准化临床应用说明
相关产品:
TKK3350型口腔功能测定仪(健口くん(口腔機能測定機器),T.K.K.3350)
文献索引(部分)
- J Oral Rehabil. 2026 May;53(5):945-959. doi: 10.1111/joor.70150. Epub 2026 Jan 16.
- Codas. 2026 Jan 26;38(1):e20240317. doi: 10.1590/2317-1782/e20240317pt. eCollection 2026.
- J Oral Rehabil. 2026 Apr 2:10.1111/joor.70190. doi: 10.1111/joor.70190. Online ahead of print.
- J Neuromuscul Dis. 2026 Mar 13:22143602261433495. doi: 10.1177/22143602261433495. Online ahead of print.
- Clin Oral Investig. 2025 Aug 12;29(9):407. doi: 10.1007/s00784-025-06483-2.
- Eur J Orthod. 2025 Dec 16;48(1):cjaf110. doi: 10.1093/ejo/cjaf110.
- J Clin Med. 2025 Jul 7;14(13):4781. doi: 10.3390/jcm14134781.
- Healthcare (Basel). 2025 Oct 2;13(19):2509. doi: 10.3390/healthcare13192509.
- J Oral Rehabil. 2025 Oct;52(10):1819-1828. doi: 10.1111/joor.13989. Epub 2025 Jun 2.
- Gerodontology. 2025 Dec;42(4):602-610. doi: 10.1111/ger.70005. Epub 2025 Jul 10.
- Biomedicines. 2026 Feb 19;14(2):465. doi: 10.3390/biomedicines14020465.
- J Orofac Orthop. 2025 Jun 24. doi: 10.1007/s00056-025-00597-8. Online ahead of print.
- BMC Geriatr. 2025 Mar 24;25(1):194. doi: 10.1186/s12877-025-05859-z.
Accuracy of tongue strength, endurance, and pressure using Iowa oral performance instrument and predictors of dysphagia in community-dwelling older adults: a cross-sectional study
- Lin CH, Chung SY, Lin CT, Hwu YJ. Effect of tongue-to-palate resistance training on tongue strength in healthy adults [published online ahead of print, 2020 Jul 26]. Auris Nasus Larynx. 2020;S0385-8146(20)30168-1. doi:10.1016/j.anl.2020.07.014
- Lee KH, Jung ES, Choi YY. Effects of lingual exercises on oral muscle strength and salivary flow rate in elderly adults: a randomized clinical trial. Geriatr Gerontol Int. 2020 Jul;20(7):697-703. doi: 10.1111/ggi.13944. Epub 2020 Jun 2. PMID: 32489001.
- Su HT, Wang LM, Yang CF, Lee LH, Brajot FX. Language, speech, and oromotor function in children with Pompe disease. Neuromuscul Disord. 2020;30(5):400-412. doi:10.1016/j.nmd.2020.03.003
- Komagamine Y, Kanazawa M, Yamada A, Minakuchi S. Association between tongue and lip motor functions and mixing ability in complete denture wearers. Aging Clin Exp Res. 2019;31(9):1243‐1248. doi:10.1007/s40520-018-1070-2
- Lee JH, Choi SY. Criteria to assess tongue strength for predicting penetration and aspiration in patients with stroke having dysphagia. Eur J Phys Rehabil Med. 2020 Aug;56(4):375-385. doi: 10.23736/S1973-9087.20.06180-8. Epub 2020 Apr 24. PMID: 32329588.
- Pizzorni N, Ginocchio D, Bianchi F, Feroldi S, Vedrodyova M, Mora G, Schindler A. Association between maximum tongue pressure and swallowing safety and efficacy in amyotrophic lateral sclerosis. Neurogastroenterol Motil. 2020 Aug;32(8):e13859. doi: 10.1111/nmo.13859. Epub 2020 Apr 26. PMID: 32337820.
- Paris-Alemany A, Proy-Acosta A, Adraos-Juarez D, Suso-Marti, La Touche R, Chamorro-Sanchez J. Influence of the Craniocervical Posture on Tongue Strength and Endurance [published online ahead of print, 2020 May 22]. Dysphagia. 2020;10.1007/s00455-020-10136-9. doi:10.1007/s00455-020-10136-9
- Van den Steen L, Baudelet M, Tomassen P, Bonte K, De Bodt M, Van Nuffelen G. The effect of tongue-strengthening exercises on tongue strength and swallowing-related parameters in chronic radiation-associated dysphagia [published online ahead of print, 2020 Apr 30]. Head Neck. 2020;10.1002/hed.26179. doi:10.1002/hed.26179
- Yano J, Yamamoto-Shimizu S, Yokoyama T, Kumakura I, Hanayama K, Tsubahara A. Effects of Tongue-Strengthening Exercise on the Geniohyoid Muscle in Young Healthy Adults. Dysphagia. 2020;35(1):110-116. doi:10.1007/s00455-019-10011-2
- Van den Steen L, De Bodt M, Guns C, Elen R, Vanderwegen J, Van Nuffelen G. Tongue-Strengthening Exercises in Healthy Older Adults: Effect of Exercise Frequency - A Randomized Trial [published online ahead of print, 2020 Feb 5]. Folia Phoniatr Logop. 2020;1-8. doi:10.1159/000505153
- Hwang NK, Kim MJ, Lee G, Yoon T, Park JS, Jung Y. Effect of tongue-strengthening training combined with a tablet personal computer game in healthy adults. J Oral Rehabil. 2020;47(5):606-612. doi:10.1111/joor.12944
- Vanderwegen J, Van Nuffelen G, Elen R, De Bodt M. The Influence of Age, Sex, Visual Feedback, Bulb Position, and the Order of Testing on Maximum Anterior and Posterior Tongue Strength in Healthy Belgian Children. Dysphagia. 2019;34(6):834-851. doi:10.1007/s00455-019-09976-x
- Van den Steen L, Vanderwegen J, Guns C, Elen R, De Bodt M, Van Nuffelen G. Tongue-Strengthening Exercises in Healthy Older Adults: Does Exercise Load Matter? A Randomized Controlled Trial. Dysphagia. 2019;34(3):315-324. doi:10.1007/s00455-018-9940-5
- Van den Steen L, Van Gestel D, Vanderveken O, et al. Evolution of self-perceived swallowing function, tongue strength and swallow-related quality of life during radiotherapy in head and neck cancer patients. Head Neck. 2019;41(7):2197-2207. doi:10.1002/hed.25684
- Steele CM, Peladeau-Pigeon M, Barbon CAE, et al. Modulation of Tongue Pressure According to Liquid Flow Properties in Healthy Swallowing. J Speech Lang Hear Res. 2019;62(1):22-33. doi:10.1044/2018_JSLHR-S-18-0229
- Saccomanno S, Di Tullio A, D'Alatri L, Grippaudo C. Proposal for a myofunctional therapy protocol in case of altered lingual frenulum. A pilot study. Eur J Paediatr Dent. 2019;20(1):67-72. doi:10.23804/ejpd.2019.20.01.13
- Potter NL, Nievergelt Y, VanDam M. Tongue Strength in Children With and Without Speech Sound Disorders. Am J Speech Lang Pathol. 2019;28(2):612-622. doi:10.1044/2018_AJSLP-18-0023
- Pitts LL, Kanadet RM, Hamilton VK, Crimmins SK, Cherney LR. Lingual Pressure Dysfunction Contributes to Reduced Swallowing-Related Quality of Life in Parkinson's Disease. J Speech Lang Hear Res. 2019;62(8):2671-2679. doi:10.1044/2019_JSLHR-S-18-0366
- Pereira TC, Furlan RMMM, Motta AR. Relationship between mouth breathing etiology and maximum tongue pressure. Relação entre a etiologia da respiração oral e a pressão máxima da língua. Codas. 2019;31(2):e20180099. Published 2019 Apr 1. doi:10.1590/2317-1782/20182018099
- Park JS, Lee SH, Jung SH, Choi JB, Jung YJ. Tongue strengthening exercise is effective in improving the oropharyngeal muscles associated with swallowing in community-dwelling older adults in South Korea: A randomized trial. Medicine (Baltimore). 2019;98(40):e17304. doi:10.1097/MD.0000000000017304
- Park JS, Hwang NK, Kim HH, Choi JB, Chang MY, Jung YJ. Effects of lingual strength training on oropharyngeal muscles in South Korean adults. J Oral Rehabil. 2019;46(11):1036-1041. doi:10.1111/joor.12835
- Park HS, Oh DH, Yoon T, Park JS. Effect of effortful swallowing training on tongue strength and oropharyngeal swallowing function in stroke patients with dysphagia: a double-blind, randomized controlled trial. Int J Lang Commun Disord. 2019;54(3):479-484. doi:10.1111/1460-6984.12453
- O'Connor-Reina C, Plaza G, Garcia-Iriarte MT, et al. Tongue peak pressure: a tool to aid in the identification of obstruction sites in patients with obstructive sleep apnea/hypopnea syndrome. Sleep Breath. 2020;24(1):281-286. doi:10.1007/s11325-019-01952-x
- Mul K, Berggren KN, Sills MY, et al. Effects of weakness of orofacial muscles on swallowing and communication in FSHD. Neurology. 2019;92(9):e957-e963. doi:10.1212/WNL.0000000000007013
- McKay R, Smart S, Cocks N. Investigating Tongue Strength and Endurance in Children Aged 6 to 11 Years [published online ahead of print, 2019 Dec 2]. Dysphagia. 2019;10.1007/s00455-019-10081-2. doi:10.1007/s00455-019-10081-2
| PN 1-3100-DL | IOPI吞咽障碍评估和训练舌压仪(豪华套装) | 电邮询价 |
| PN 1-3100-SD | IOPI吞咽障碍评估和训练舌压仪(标准套装) | 电邮询价 |
| PN 1-3200 | IOPI吞咽障碍评估和训练舌压仪(训练套装) | 电邮询价 |
| PN 5-6010 | 标准舌压测量球囊(适用于,豪华套装和标准套装)—1盒10个 | 电邮询价 |
| PN 5-6105 | 训练用舌压测量球囊(适用于,训练套装)—1盒5个 | 电邮询价 |
| PN 5-0001 | 连接管(适用于,豪华套装和标准套装) | 电邮询价 |
| PN 5-8101 | IOPI报告生成单元 | 电邮询价 |
| PN 5-3001 | 橡胶面部模型 | 电邮询价 |
| PN 800-3102 | 患者进展数据表,15张 | 电邮询价 |
| PN 800-3103 | 舌头压力测量球囊定位表 | 电邮询价 |
| PN 800-3203 | 培训治疗师-患者使用说明;15张 | 电邮询价 |
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
iowa oral performance instrument,IOPI Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. Clinical Importance Knowing a patient’s tongue strength is clinically useful for several reasons: DECIDING whether tongue weakness is involved in oral stage swallowing problems and/or dysarthria: If the tongue is weak, you can start tongue strengthening therapy. If the tongue strength is normal, you can eliminate weakness as a cause of the swallowing or speech problems, and thus concentrate on other more useful therapies. DOCUMENTING that a patient’s tongue is weak, and therefore that strengthening exercises are justified. This may be important to insurance providers and administrators who are concerned with the cost of delivering such therapy. ASSESSING the results of tongue strengthening therapy over time: If tongue strength doesn’t increase over time, then perhaps the patient is not performing the prescribed exercises, or not doing them forcefully enough. If the tongue strength does increase, even a little bit, it can be "rewarding" for the patient to see concrete evidence improvement. EXERCISING the patient’s tongue. Performing tongue exercise using an IOPI® can give the patient very specific "targets" to achieve with their efforts, and give them immediate feedback about improvement. Pressure as a Measure of Strength Measuring the maximum pressure that a person can produce by squeezing a compliant bulb against the hard palate to estimate the strength of the tongue was a completely novel idea when the IOPI was patented in 1992. Since that time, many research studies have been published that have used the IOPI or IOPI-like instruments to measure tongue strength (see Publications). Tongue Exercise using BIOFEEDBACK Evidence exists to show that tongue exercise in dysphagia patients, as documented with the IOPI, can lead to improved swallowing outcomes. The IOPI allows the clinician to use protocols that have been proven to work in exercise science. The clinician sets the target pressure on the IOPI’s biofeedback light array and instructs the patient to squeeze the bulb until they turn the top green light on. The patient is visually reinforced for hitting their target. Tongue Elevation Strength Tongue elevation strength is the maximum pressure of the tongue pressing against the hard palate. The IOPI measures this when the Tongue Bulb is placed in the “anterior” position – the hard palate just behind the alveolar ridge. The image to the right shows this position. You can simulate this placement if you suck on your thumb: the pad of your thumb will be pressing against the hard palate behind the alveolar ridge and your tongue will be pressing on your thumbnail instead of a Tongue Bulb. Most published reports on tongue strength have used the IOPI with the Tongue Bulb in the “anterior” position. Therefore, there is a great deal of information, derived from many different laboratories and clinics, about tongue elevation strength. This information suggests the following generalization: Repeated measurements of tongue strength in the same individual are quite reliable, particularly after the patient has done the task a few times. There is considerable variability in tongue strength in a population of adults reporting no swallowing or speech problems (see Normal Values). There is a clear central tendency, however, with an average maximum pressure of about 60 kPa, and a range of 40-80 kPa. Patients with oral phase swallowing problems have a tongue strength that is significantly lower than the normal population. LIP STRENGTH Why Measure Lip Strength? Inadequate lip strength may contribute to problems with deglutition, such as food containment during chewing. If lip weakness is severe, it also may interfere with the production of plosive speech sounds. Such weakness would probably be obvious, but being able to accurately "track" the degree of weakness would enable the clinician to determine whether the weakness is getting better or worse, and/or determine if training improves lip strength. Additionally, observing lip weakness in a patient may help identify abnormalities within the nervous system such as subtle cortical dysfunction, or disease processes gradually affecting the function of the facial nerve. Lip Strength Measurement To measure lip strength, an IOPI bulb is placed inside the cheek just lateral to the corner of the mouth and the patient squeezes the IOPI bulb against the buccal surface of the teeth by pursing the lips as hard as possible. Although the bulb is not directly between the lips, it is valid because the pressure developed in the bulb depends upon the strength of the circumferential muscle complex that surrounds the mouth, in particular the obcularis oris. It is tension in these muscles that allows the lips to be compressed against one another. IOPI® PRO - Deluxe Kit PN 1-3100-DL INCLUDES: 1 IOPI Pro 1 Pro Carrying Case 5 Tongue Bulbs 1 Connecting Tube 1 Accuracy Check Kit 1 Set of AA batteries 1 User Manual Patient Progress Datasheets (15 page pad) Tongue Bulb Positioning Sheet 2-year warranty Plus: • 1 IOPI Report Generator • 1 Additional Connecting Tube IOPI® TRAINER KIT PN 1-3200 INCLUDES: 1 IOPI Trainer 1 Trainer Carrying Case 5 Trainer Bulbs 1 Set of AA batteries 1 User Manual Trainer Patient Instructions 2-year warranty TONGUE BULBS (Pro & Series 2 Devices) - Box of 10 PN 5-6010 TRAINER BULBS (Trainer Device) - Box of 5 PN 5-6105 CONNECTING TUBE (Pro & Series 2 Devices) PN 5-0001 IOPI® REPORT GENERATOR PN 5-8101 INCLUDES: 1 IOPI Report Generator Software (PC-based) 1 USB Drive 1 Mini-USB to USB Cable RUBBER FACE MODEL PN 5-3001 Useful for demonstrating bulb placement Fits in Pro Carrying Case pouch Dimensions: 8" x 6" x 3/8" PATIENT PROGRESS DATASHEETS (15 page pad) PN 800-3102 TONGUE BULB POSITIONING SHEET PN 800-3103 TRAINER PATIENT INSTRUCTIONS (15 page pad) PN 800-3203
相关产品
